Warnings and precautions
Impaired ability to drive or engage in other potentially hazardous activities
- ZURZUVAE causes driving impairment due to central nervous system (CNS) depressant effects1
- Advise patients not to drive a motor vehicle or engage in other potentially hazardous activities requiring complete mental alertness, such as operating machinery, until at least 12 hours after ZURZUVAE administration for the duration of the 14-day treatment course. Inform patients that they may not be able to assess their own driving competence or the degree of driving impairment caused by ZURZUVAE1
Central nervous system depressant effects
- ZURZUVAE can cause CNS depressant effects such as somnolence and confusion1
- Somnolence developed in 36% of patients who received ZURZUVAE (50 mg) and in 6% of patients who received placebo daily. Some ZURZUVAE-treated patients developed confusional state. One of these cases was severe, and was also associated with somnolence, dizziness, and gait disturbance1
- A higher percentage of ZURZUVAE-treated patients, compared to placebo-treated patients, experienced somnolence, dizziness, or confusion that required dosage reduction, interruption, or discontinuation1
- Because ZURZUVAE can cause CNS depressant effects, patients may be at higher risk of falls1
- Other CNS depressants such as alcohol, benzodiazepines, opioids, tricyclic antidepressants, or drugs that increase zuranolone concentration, may increase impairment of psychomotor performance or CNS depressant effects such as somnolence, cognitive impairment, and the risk of respiratory depression in ZURZUVAE-treated patients1
- To reduce the risk of CNS depressant effects and/or mitigate CNS depressant effects that occurs with ZURZUVAE treatment:
- If patients develop CNS depressant effects, consider dosage reduction or discontinuation of ZURZUVAE1
- If use with another CNS depressant is unavoidable, consider dosage reduction1
- Reduce the ZURZUVAE dosage in patients taking strong CYP3A4 inhibitors1
Suicidal thoughts and behavior
- In pooled analyses of placebo-controlled trials of chronically administered antidepressant drugs (SSRIs and other antidepressant classes) that included approximately 77,000 adult patients and 4,500 pediatric patients, the incidence of suicidal thoughts and behaviors in antidepressant-treated patients age 24 years and younger was greater than in placebo-treated patients. There was considerable variation in risk of suicidal thoughts and behaviors among drugs, but there was an increased risk identified in young patients for most drugs studied. There were differences in absolute risk of suicidal thoughts and behaviors across the different indications, with the highest incidence in patients with major depressive disorder (MDD)1
- ZURZUVAE does not directly affect monoaminergic systems. Consider changing the therapeutic regimen, including discontinuing ZURZUVAE, in patients whose depression becomes worse or who experience emergent suicidal thoughts and behaviors1
Embryo-fetal toxicity
- Based on findings from animal studies, ZURZUVAE may cause fetal harm when administered to a pregnant woman1
- Advise a pregnant woman of the potential risk to an infant exposed to ZURZUVAE in utero. Advise females of reproductive potential to use effective contraception during treatment with ZURZUVAE and for one week after the final dose1
Adverse reactions
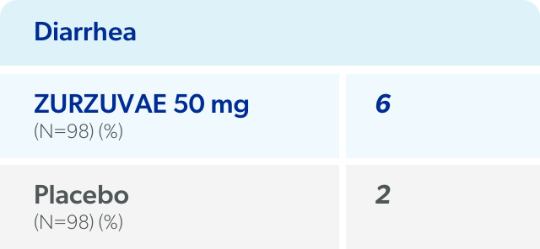
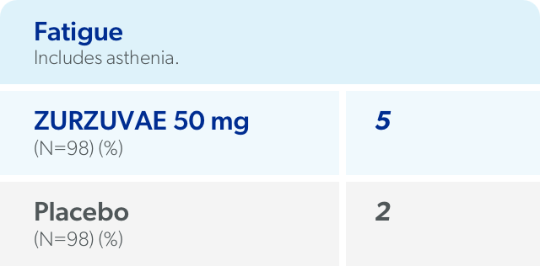
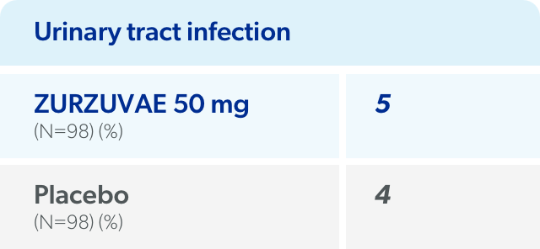
The most common adverse reactions with ZURZUVAE 50 mg1
(≥5% and greater than placebo)
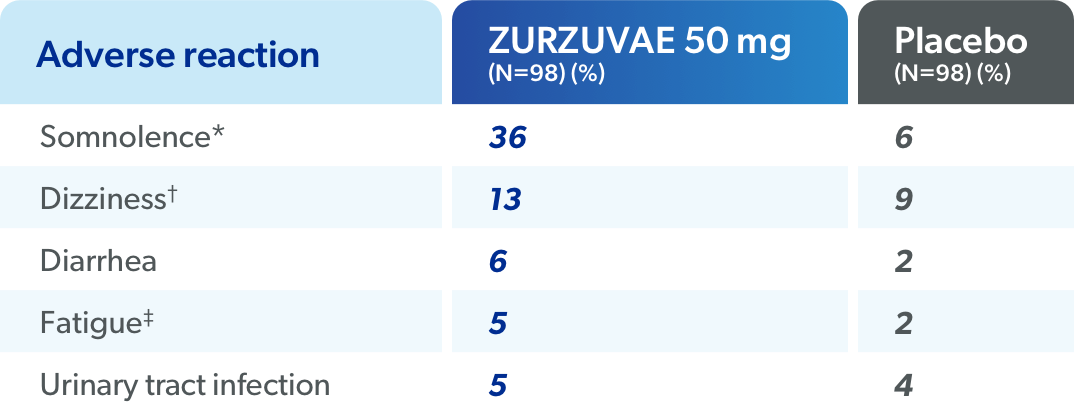
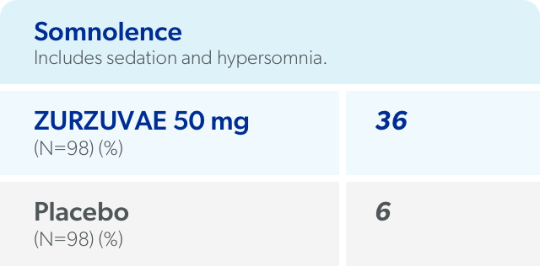
*Includes sedation and hypersomnia.
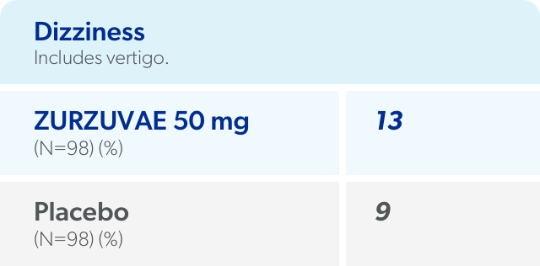
†Includes vertigo.
‡Includes asthenia.
In a study of another capsule formulation ≈40 mg, the most common adverse reactions (≥5% and greater than placebo) in ZURZUVAE-treated patients were somnolence, nasopharyngitis, dizziness, fatigue, and diarrhea.1
Across PPD clinical studies at all doses studied, serious adverse reactions included confusional state (1%)1
Dosage reduction due to an adverse reaction in patients treated with ZURZUVAE 50 mg1

The most common adverse reactions leading to dosage reduction in ZURZUVAE-treated patients were somnolence (10%) and dizziness (6%)1
Discontinuation due to adverse reactions1


The most common adverse reaction leading to treatment discontinuation in ZURZUVAE-treated patients was somnolence1
Pregnancy and lactation
Pregnancy
Advise pregnant women of the potential risk to the fetus1
- Based on findings from animal studies, ZURZUVAE may cause fetal harm when administered to a pregnant woman1
- Available data on ZURZUVAE use in pregnant women are insufficient to evaluate for a risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes1
- Healthcare professionals are encouraged to register patients taking ZURZUVAE with the National Pregnancy Registry for Antidepressants, which monitors pregnancy outcomes in women exposed to antidepressants, at 1-844-405-6185 or online at https://womensmentalhealth.org/research/pregnancyregistry/antidepressants/
- Advise patients to:
- Notify their healthcare provider if they become pregnant or intend to become pregnant during ZURZUVAE treatment1
- Use effective contraception while taking ZURZUVAE and for one week after the final dose1
Lactation
Available data from a clinical lactation study indicate ZURZUVAE is present in low levels in human milk1§
- At steady state (Day 5), the calculated maximum relative infant dose for ZURZUVAE was <1%1
- There are no data on the effects of ZURZUVAE on a breastfed infant and limited data on the effects on milk production1
§A steady-state milk study was conducted in 14 healthy lactating women treated with ZURZUVAE 30 mg for 5 days.1
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ZURZUVAE and any potential adverse effects on the breastfed child from ZURZUVAE or from the underlying maternal condition1
Schedule IV information
ZURZUVAE contains zuranolone, a Schedule IV controlled substance1
ZURZUVAE has abuse potential with associated risks of misuse, abuse, and substance use disorder including addiction1
- Individuals with a history of drug abuse or substance use disorders may be at a greater risk of these outcomes with ZURZUVAE1
- ZURZUVAE demonstrated dose-dependent abuse potential comparable to alprazolam and greater abuse potential vs placebo on positive subjective measures of “drug liking,” “overall drug liking,” “take drug again,” “high,” and “good drug effects”1||
- Dose dependent, abuse-related adverse reactions, including euphoric mood, feeling drunk, and somnolence, were reported with ZURZUVAE1||
||In a human abuse potential study, single oral doses of 30 mg, 60 mg, and 90 mg of ZURZUVAE (0.6, 1.2, and 1.8 times the recommended daily dose, respectively) were compared to single oral doses of alprazolam (1.5 mg and 3 mg) and placebo in healthy, nondependent individuals with a history of recreational CNS depressant use.1
ZURZUVAE may produce
physical dependence
- Adverse reactions reported upon discontinuation of ZURZUVAE in healthy subjects who received 50 mg of ZURZUVAE for 5 to 7 days (on the 7th day subjects received 50 mg or 100 mg) included: insomnia, palpitations, decreased appetite, nightmare, nausea, hyperhidrosis, and paranoia. These adverse reactions were mild-to-moderate in severity1
Advise patients that ZURZUVAE has abuse potential with associated risks of misuse, abuse, and substance use disorder including addiction and that ZURZUVAE is associated with the potential for physical dependence1